Obesity, can we blame it on hormones?
I put a post out last week where I highlighted the connection between neck pain and abdominal obesity. This made me think more about the topic as I see the expanding waistlines of many of my friends and most of my family.
This trend scares me….literally…I recently had a friend come and stay with me who I hadn’t seen for 15 years. Part of the reason we spent time with each other after so long was that he wanted to address his weight gain. We ended up playing a game of pickleball, like miniature tennis, and he struggled with his fitness, and I genuinely thought he could have a heart attack.
Images of me calling his wife flashed through my head, and I felt stupid for pushing him during the game. Luckily my fears weren’t realized, but this problem will only worsen.
In the US, the number of obese people is expected to rise to just under 50% by 2030 (1). This public and personal health crisis must be addressed on an individual and, where possible, at a general level.
There are different types of obesity, and the one I mentioned above, central obesity, is more serious regarding related increases in many health problems and early death. (2)
Some forms of obesity can come from hormonal changes, but the percentage of cases of hypothyroidism, Cushing, and Hypogonadism don’t explain the rapid increase in patients over the last 30 years.
However, we are learning now through research that excess body fat changes hormones which can make it hard to lose weight, but these hormonal changes are a consequence, not a cause, as they tend to normalize with weight loss (4).
Doctors aren’t equipped or trained well in advising patients on how to lose weight, and most tend to ignore it, pushing the problem, increased risk of diabetes, heart attacks, strokes, and some cancers further down the line.
Some people might think it’s easy for me to talk about obesity because I’m slim and have some sort of genetic ability to stay thin. Well, genetics play a small role in obesity but as everyone who has ever spent time with me says…” You don’t eat enough .” My usual reply is that I eat the right amount, considering I’m about the same weight I was 20 years ago.
Yet, when I spend time in Canada or the UK on holiday, I put on weight, usually about 5-10lbs in a month. That’s mainly because I’m eating out or people are cooking for me, and I’m not in complete control of what I’m eating as I am at home. If I stayed a year with no change in those eating habits, I might just put on 30 lbs, and that’s what I see with my peer group once skinny athletic men are now walking around with their rotund waistlines as a source of pride, maybe even status.
The question for me is how do I bring up the topic of weight gain or loss without being accused of fat shaming?
When patients come to me for advice, it’s easy I use a lifestyle medicine approach which allows me to help patients and clients see the connection between things that are not commonly discussed as causes of obesity, namely,
Disrupted sleep pattern (5)
Timing of food eaten (6)
Stress levels and how to manage them (7)
Environment (3)
But when it’s my friends, do I stand by and ignore the fact that some support and encouragement may be the key to preventing stroke, heart attack, and some cancers?
You see, the environment is a particular concern of mine. As mentioned, I’ve seen how obesity can spread through social networks. I’ve seen certain groups of people collectively become obese over the years. The study quoted here highlights this very well,
“The study found that when an individual becomes obese, the chances that a friend of theirs will become obese increase by 57 percent. Their siblings have a 40 percent increased risk of obesity, and their spouse a 37 percent increased risk”.
Obesity is a multifactorial problem that needs to be addressed in a multifactorial way.
Hormones play a small role in the current epidemic. Still, solid support from healthcare practitioners can help people tackle this problem and save lives, unnecessary suffering, and money.
Sources:
(1)
https://www.nejm.org/doi/full/10.1056/NEJMsa1909301?query=featured_home
(2)
https://www.hsph.harvard.edu/obesity-prevention-source/obesity-causes/
(3)
https://www.endocrine.org/patient-engagement/endocrine-library/obesity
(4)
https://www.ncbi.nlm.nih.gov/books/NBK279053/
https://www.endocrine.org/patient-engagement/endocrine-library/obesity
(5)
https://www.hsph.harvard.edu/nutritionsource/sleep/
(6)
https://www.hsph.harvard.edu/nutritionsource/healthy-weight/diet-reviews/intermittent-fasting/
(7)
https://www.amymyersmd.com/article/cortisol-and-weight-gain/
(8)
https://hms.harvard.edu/news/obesity-spreads-through-social-networks
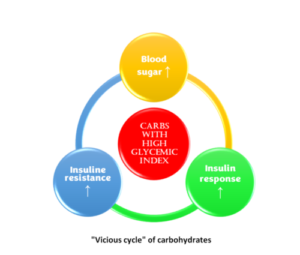 When this cycle starts, the second fact comes into the picture. Insulin stimulates the conversion of blood glucose to fat, lipogenesis, and the fat that travels in the blood is called triglycerides; too much of that is the second criterion for diagnosing metabolic syndrome. The third fact is that insulin also slows down the body’s ability to use fat as a fuel source (lipolysis), so insulin promotes the growth of fat and prevents fat burning; hence, it is stored waistlines increase.
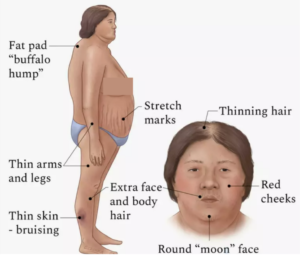
The last fact is that cortisol is a stress hormone that raises blood sugar, leads to insulin resistance, and is very closely associated with belly fat. For example, if a person has too much cortisol, a condition known as Cushing syndrome, they will develop insulin resistance, belly fat, and typical body shapes, as shown in the diagram.
When this cycle starts, the second fact comes into the picture. Insulin stimulates the conversion of blood glucose to fat, lipogenesis, and the fat that travels in the blood is called triglycerides; too much of that is the second criterion for diagnosing metabolic syndrome. The third fact is that insulin also slows down the body’s ability to use fat as a fuel source (lipolysis), so insulin promotes the growth of fat and prevents fat burning; hence, it is stored waistlines increase.
The last fact is that cortisol is a stress hormone that raises blood sugar, leads to insulin resistance, and is very closely associated with belly fat. For example, if a person has too much cortisol, a condition known as Cushing syndrome, they will develop insulin resistance, belly fat, and typical body shapes, as shown in the diagram.
 If we correlate the five risk factors with carbs, insulin, and cortisol, we can establish that:
If we correlate the five risk factors with carbs, insulin, and cortisol, we can establish that:

